The role of intellectual property rights on access to medicines in the WHO African region 30 years after the TRIPS agreement.
The article examines the impact of the TRIPS Agreement on global intellectual property protection, focusing on access to medicines. It discusses challenges such as higher drug prices and barriers to generic production, while also exploring alternative models like PDPs. The article highlights constraints in the WHO African Region, including limited financing and regulatory issues, and emphasizes recent tensions between IPP and access to medicines in light of public health emergencies like Ebola and COVID-19.
Introduction:
The adoption of the TRIPS Agreement in 1994 by WTO Member States significantly impacted global intellectual property protection (IPP), particularly in access to medicines. Effects include higher prices of medicinal products, hindrance to local manufacture of generics, and delayed market entry for generic products.
While IPP incentivizes pharmaceutical R&D investment, it fails to address neglected diseases prevalent in developing countries. Alternative models like PDPs and leveraging TRIPS flexibilities aim to address this issue. However, access to medicines in the WHO African Region is also constrained by factors like limited public financing, logistical challenges, and inadequate regulatory frameworks.
Recent public health emergencies like Ebola and COVID-19 further highlight tensions between IPP and access to medicines. For instance, Gilead Sciences' application for orphan drug status for remdesivir, later rescinded, underscored these tensions. Gilead's subsequent non-exclusive licensing agreements aim to expand access to remdesivir in low and middle-income countries, including those in the WHO African Region.
WHO, intellectual property and access to medicines :
The intersection of access to medical products, research and development (R&D) in rare and tropical diseases, and trade has been a focus of the World Health Organization (WHO) since 1996. The WHO's mandate in this regard was initially articulated in a World Health Assembly (WHA) resolution on the Revised Drug Strategy in 1996. This resolution tasked the WHO Director-General with supporting Member States in improving access to essential drugs, promoting R&D for rare and tropical diseases, and assessing the impact of the World Trade Organization (WTO) on national drug policies.
Over time, this mandate has been reinforced through subsequent WHA resolutions. In 2003, WHO member states established a Commission on Intellectual Property Rights, Innovation and Public Health (CIPIH), which recommended the development of a global plan of action to enhance funding for products addressing diseases affecting developing countries. This led to the adoption of the GSPOA-PHI in 2009, and the initiation of the WHO-WIPO-WTO trilateral cooperation.
Resolutions in 2018 and 2019 called for the elaboration of roadmaps and implementation plans outlining WHO's work on access to medicines and vaccines, consistent with the GSPOA-PHI. Additionally, efforts have been made to improve the transparency of markets for health products, including promoting publicly available patent status information databases
Role of WIPO and Technical assistance for the implementation of TRIPS:
In the collaborative framework of the WHO-WIPO-WTO trilateral cooperation, the three agencies work cohesively to fulfill their individual mandates while ensuring efficient use of resources and avoiding duplication of efforts. WIPO, guided by the 1995 Agreement with WTO and recommendations from the WIPO Development Agenda, provides crucial technical assistance to developing countries for TRIPS Agreement implementation. This assistance, characterized by a developmental focus and tailored to specific needs, has been extended to 24 countries in the WHO African Region for the development of national IP strategies and legislative support, although some countries such as Gabon, Ghana, and South Sudan have yet to benefit from such assistance.
Meanwhile, within this trilateral collaboration, WHO and WTO contribute to broader health and trade initiatives, respectively, further complementing efforts to address global health challenges while navigating intellectual property issues. This collaborative approach underscores the importance of coordination and partnership among international organizations in fostering equitable access to medicines and promoting sustainable development worldwide.
The intellectual property regulation and governance landscape in the WHO African region:
Countries in the WHO African Region navigate a complex intellectual property (IP) regulatory environment influenced by global and regional frameworks. The Paris Convention for the Protection of Industrial Property (1883) and the Agreement on Trade-Related Aspects of Intellectual Property Rights (TRIPS Agreement) (1994) form the basis of the global IP framework. While most countries in the region (40 out of 47) are WTO members and adhere to the TRIPS Agreement, they retain flexibility in implementing it within their legal systems.
Some countries, such as Algeria, Comoros, Equatorial Guinea, Eritrea, Ethiopia, Sao Tome and Principe, and South Sudan, are not WTO members but are in accession discussions. At the regional level, countries are affiliated with either the Harare Protocol on Patents and Industrial Design (administered by ARIPO) or the Bangui Agreement (administered by OAPI), further adding to the complexity of IP regulation in the region
The African Regional Intellectual Property Office (ARIPO):
It operates as a collaborative body established under the Lusaka Agreement in 1976, comprising 20 member states, 18 of which belong to the WHO African Region. ARIPO's mission centers on harmonizing and developing intellectual property laws among its members to address their specific needs and foster collaboration on IP-related activities. The Harare Protocol on Patents and Industrial Designs, adopted in 1982 and enforced in 1984, serves as a mechanism within ARIPO for regional patent filing, examination, and granting across various technological fields, including pharmaceuticals. However, concerns arise regarding the implementation of TRIPS flexibilities, particularly in patentability criteria extending to pharmaceutical products and the lack of provisions for patent opposition, potentially facilitating frivolous patent claims.
Organisation Africaine De La Propriété Intellectuelle (OAPI):
Established by the Bangui Agreement in 1977, aims to administer uniform administrative procedures for industrial property protection among its member states. OAPI functions as both a national and central patent documentation body for its members, facilitating patent applications designated for protection across all OAPI member countries. The patentability criteria under the Bangui Agreement broadly encompass pharmaceutical products and processes. However, unlike ARIPO, OAPI operates solely as a formality examination office, granting patents based on meeting formality requirements without substantive examination. This absence of a patent opposition system raises concerns regarding the potential for invalid or frivolous patents within the OAPI system.
Conclusion:
In conclusion, the experiences stemming from the HIV/AIDS pandemic in the 1990s and the recent global efforts to combat COVID-19 have brought to light the intricate relationship between intellectual property rights and public health interests. These experiences have prompted a learning curve, evident in actions taken by pharmaceutical companies like Gilead Sciences, which have shown a willingness to engage in voluntary licensing agreements with manufacturing firms in developing countries. Such agreements aim to cater to less affluent markets and ensure broader access to essential medications.
Furthermore, the swift response of countries such as Canada, Germany, Chile, and Ecuador in amending their patent laws to restrict market exclusivities and facilitate compulsory licensing, if deemed necessary, for COVID-19 medicinal products, serves as a testament to the adaptability of TRIPS flexibilities in addressing urgent health needs. This demonstrates a growing recognition of the need to balance intellectual property rights with public health imperatives during times of crisis.
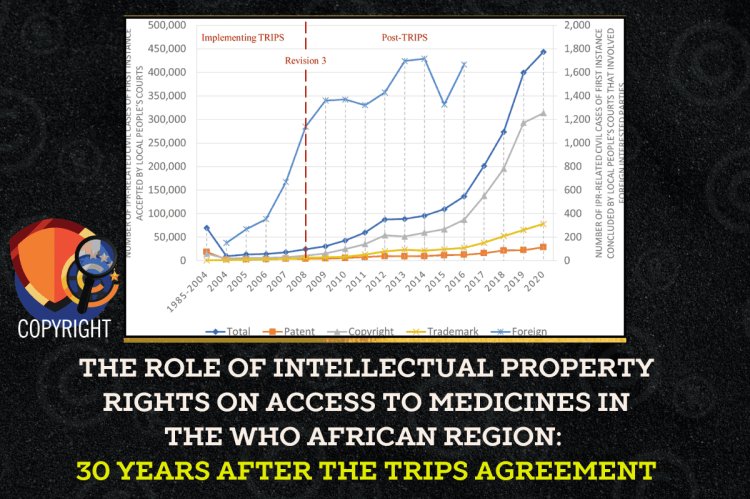
In the African Region, the relatively low levels of patenting activity underscore the pressing need to bolster health innovation systems. Achieving this entails implementing policies that support robust health research systems and establishing a local incentive structure aimed at directing research efforts towards addressing endemic health challenges. Additionally, efforts should focus on developing local scientific and biomedical research capacities, as well as enhancing local manufacturing capabilities. By prioritizing these aspects, African countries can strengthen their ability to respond to health crises effectively and meet the healthcare needs of their populations more comprehensively.












